
Cause, Ideology & Treatment Options

Scoliosis is the most common deformity of the spine and often consists of lateral displacement with associated rotation of the vertebral bodies (7).The term scoliosis is a condition first described in detail by the Greek physician Hippocrates who took its name from the Greek word 'scolios' meaning 'crooked' (7). A scoliosis is normally considered if there is a Cobb angle (explained below) of at least ten degrees of spinal angulation with lateral curvature shown on a posterior-anterior radiograph (5).
As the UK Scoliosis Association highlights, scoliosis is neither infectious nor contagious, but can develop at any age and usually becomes most clinically evident during growth, growth spurts or rapid somatic growth especially during puberty (7). The condition is classified broadly as congenital, neuromuscular, syndrome-related, idiopathic and spinal curvature due to secondary reasons (5).
Presently, the cause of scoliosis is thought to be multifactorial, but 80% of cases are largely idiopathic (undetermined cause) (1, 11).
The different stages of occurrence are as follows:
- Before birth (congenital)
- Infantile (0-3 years); structural malformation that more commonly affects boys than girls with most cases developing within the first year of life and tending to have a leftward trending curvature (levoscoliosis) (6).
- Young children; juvenile (4-10 years)
- Older Children; adolescent idiopathic scoliosis (AIS) (11-18 years) more commonly developed in girl and involves a structural curvature that commonly has a rightward trend (dextroscoliosis) (5, 6).
- Adults (degenerative or de novo)
The classification of scoliosis is dependent upon which region of the spine is affected with usually being termed either 'thorcaic', 'lumbar' or 'thoracolumbar' and the involvement of any of these areas is of significance as one must take organ function into consideration. For instance, the thoracic spine is primarily responsible for the respiratory and cardiovascular complications of scoliosis (7). A lumbar spine scoliotic pattern can later affect an individual's pelvic floor strength, incontinence or cause bowel and bladder related pathology or disorder (8).
It has been postulated that the condition might be related to proprioception or homeostasis disorders along with inheritance or genetics as well as metabolic, hormonal and biomechanical factors (1). It is worth noting that biomechanical or hormonal disturbances can cause reduced vertebral bone mass which can further progress spinal curvature (2).
The Nature of the Scoliosis
A scoliosis is classified with accordance to the side of its occurrence into either left or right sided curves and each curve of a scoliosis is classified as either having a convex or concave side as well as a primary curve and a secondary curve (10). The primary curve is usually stiffer and the curve site is classified with accordance to the location of the apical or apex vertebra in the coronal plane within either the cervical, thoracic or lumbar spine (6).
Locations & Types of Scoliosis: Dextroscoliosis & Levoscoliosis
Dextroscoliosis
is abnormal sideways curvature of the spine laterally displaced to the right and also known as a dextrocurvature
(6) .
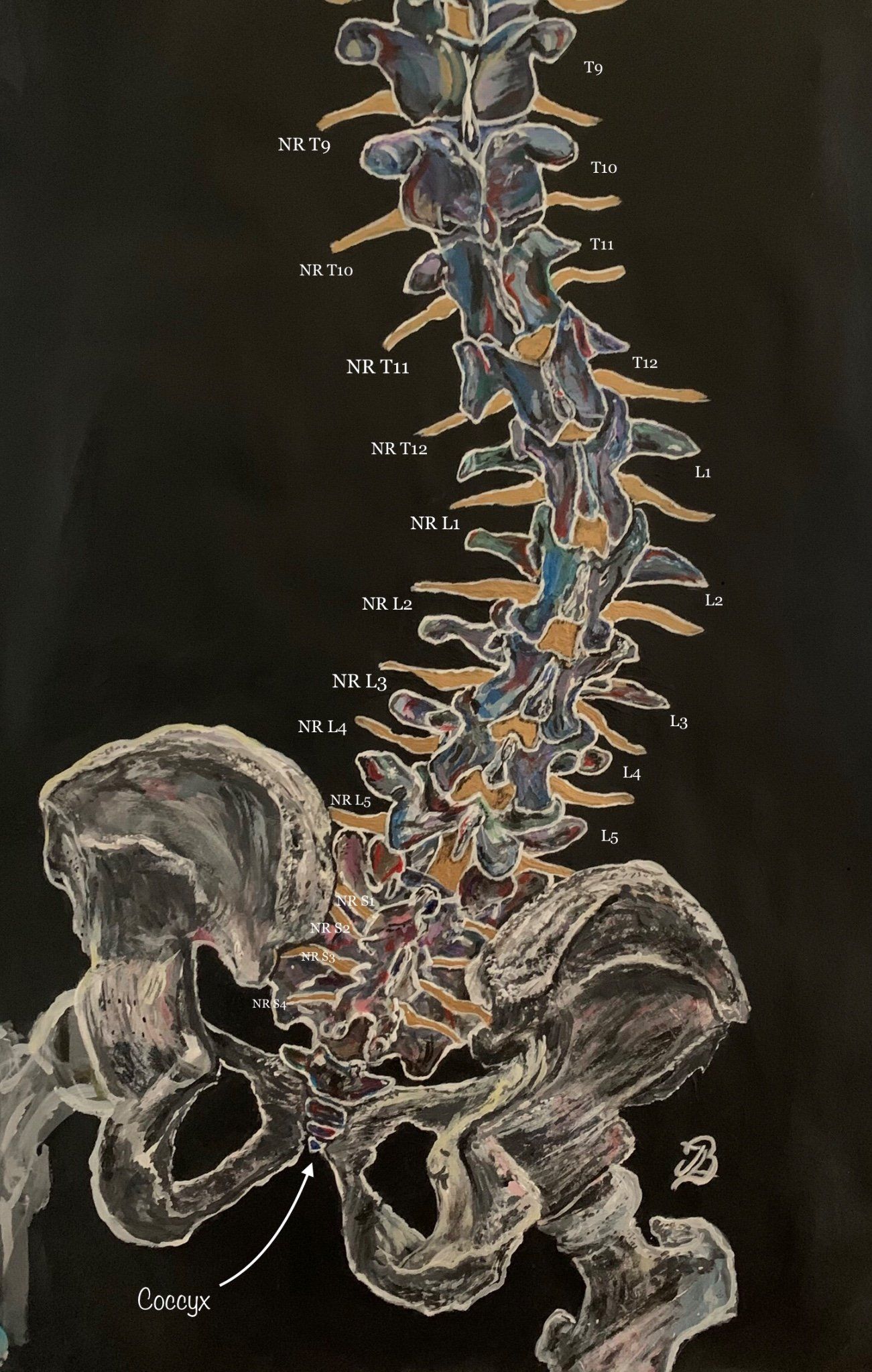
The above picture (Figure 1) shows a lumbar dextroscoliosis
which characterises an S-shaped curvature of the spine, specifically the lumbar region.
Thoracic dextroscoliosis
is an abnormal curvature within the thoracic region of the spine that also curves laterally to the right.
When a spinal curve deviates to the left, it is known as levoscoliosis
or levocurvature
. A levoscoliosis can affect either the lumbar or thoracic regions of the spine and known as a thoracic levoscoliosis
and lumbar levoscoliosis
respectively (10).
Structural or Non Strucutral Scoliosis
Structural:
Scoliosis may be structural
which is when the patient's spine has an anatomical physical curve that can be observed whilst the patient is standing or sitting.Because of vertebral morphologic changes (eg, wedging and rotation), a structural curve is not correctable with ipsilateral bending or whilst curving to the same side (6).
Structural scoliosis can be idiopathic which tends to affect girls during adolescence more so than boys. A UK study found that scoliosis in girls over 8 years of age outnumbered boys by almost 3 to 1 (Nnadi, 2018). Idiopathic scoliosis can be further classified into infantile, juvenile and adolescent types or early and late onset (1,2).
Structural scoliosis can also be secondary to congenital or neurological disorders (e.g. cerebral palsy or paralysis), neuromuscular conditions, (e.g. Duchenne muscular dystrophy), tumours, trauma, syndromic conditions (e.g. Marfans syndrome and neurofibromatosis) (5).
Non Structural:
Also known as a functional scoliosis with the latter to be caused from conditions such as lower limb disorders such as limb length discrepancy, herniated discs, hip dysplasia or limb deficiency syndromes (1).
By contrast,
no vertebral morphologic changes take place in a
non structural curve, which is a mild compensatory curve that can be corrected during ipsilateral
bending (4, 6). A non structural curve does not usually
progress.
Cobb's Angle
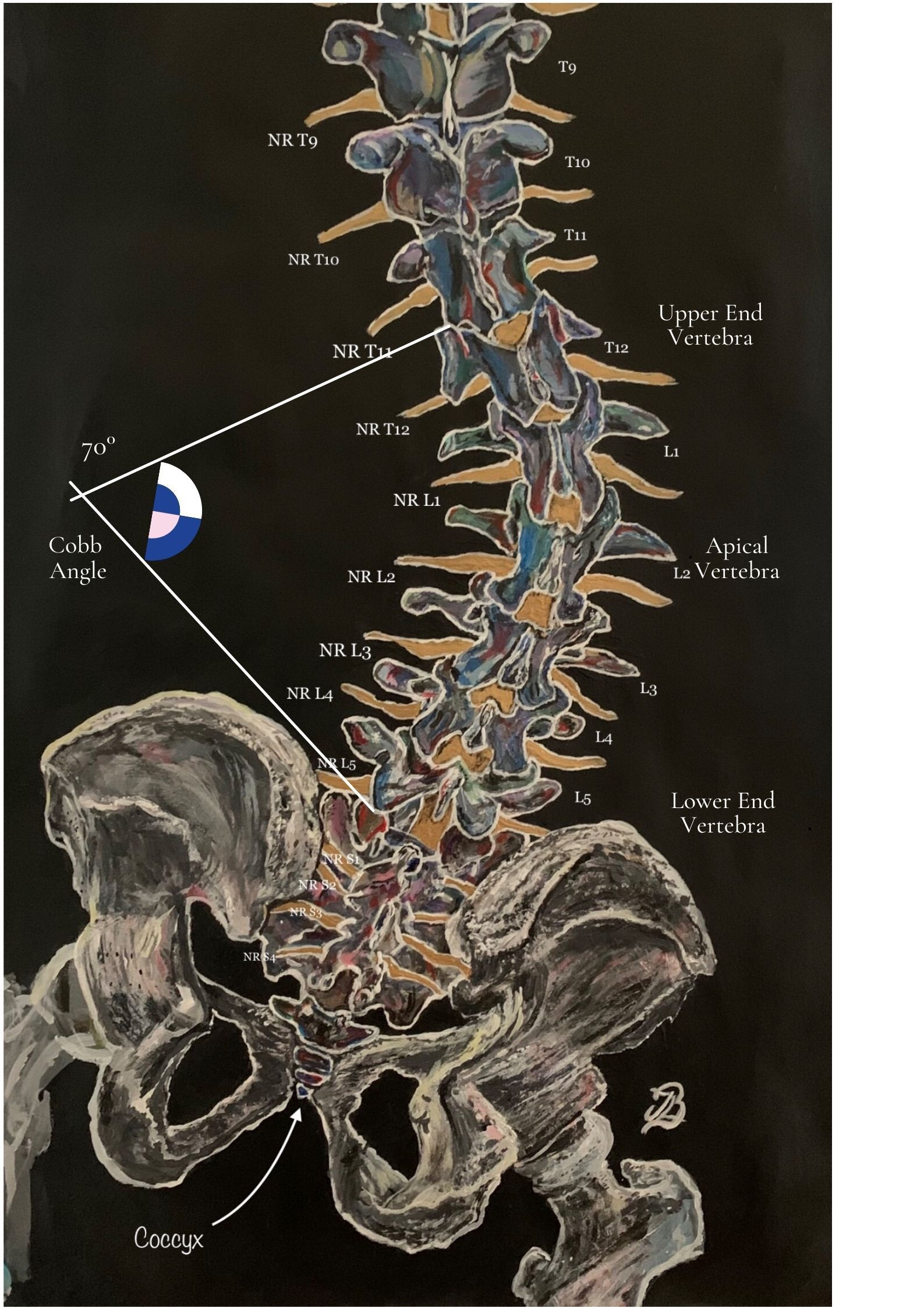
The Cobb angle is useful for assessing initial stages of a scoliotic curve, its increasing magnitude and helping to decide whether it appropriate to operate or not (4, 6). The size of the curve within a scoliosis is assessed via the measurement of the cobb angle which is formed via the intersection of two lines drawn perpendicular to the transverse axes containing the upper (or superior) end vertebra and lower (inferior) end vertebra.
Thus, the upper or lower end vertebra are the most cephalad and caudal whose superior and inferior surfaces have the most maximal tilt towards the concavity of the spinal curve (which is either concave or convexed).Where the two lines intersect is the cobb angle and is measured using specialised computer software.
The vertebra or disc with the greatest rotation or farthest deviation from the centre of the vertebral column is identified as the apex or apical vertebra. The end vertebrae have maximal tilt towards the apex of the curve and are used to measure the Cobb angle (6).
A progressive curve that
requires management is defined by a Cobb angle
increase of 5° or more between consecutive radiographic examinations (6).
Kim et al., (2010) highlight that the Cobb angle measurement has limitations with that it is performed via using a two dimensional radiographic image of a three dimensional deformity and does not take rotation into account .
Adolescent and Infantile ScoloisisAdolescent and Infantile Scoloisis
Infantile and juvenile idiopathic curves
Infantile and Juvenile
are terms used to describe curves that develop from ages 0 to 3
years and 4 to 10 years of age respectively. More recently the term “early
onset’ has been used to classify curves that develop before the
age of 10 years. (4).
Although not (yet) proven, the rate or severity of scoliosis between boys and girls during prepubertal and pubertal stages in girls might be associated with hormonal factors (in particular growth hormone) (7).
Conditions such as Chiari malformations, syringomyelia and spinal cord tethering are important
associations with congenital and early onset scoliosis.
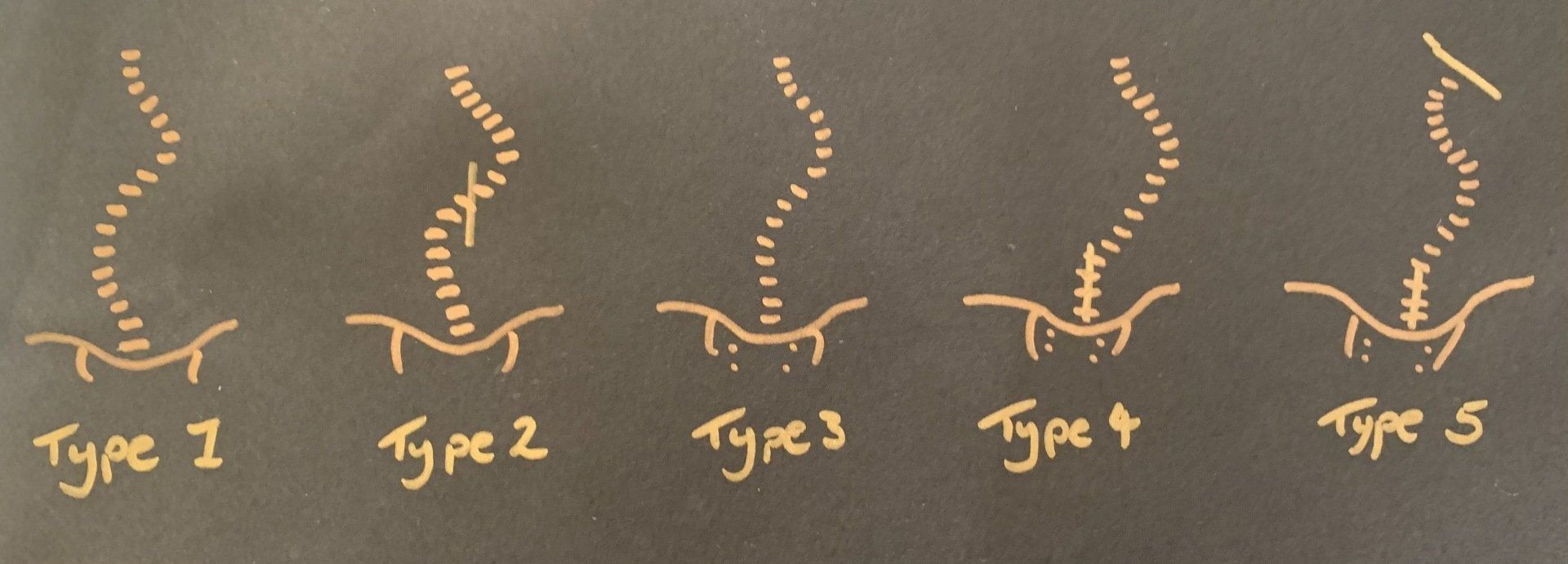
In the 1980s, adolescent idiopathic curves have been classified by King and Moe who found that there are five distinct curve patternsbased on standing radiographs of the spine (Figure 3.) (4). The aim of
this system was to determine a reliable method for selecting vertebrae for fusion (4). The curve types were stratified from I-V with type II and
III being most common. Type II is a thoracolumbar curve
while Type III is a thoracic curve.
Critique for the use of this system state that there is poor intra/inter
observer reliability with this system as curves in the coronal plane are only assessed and it fails to address lumbar/thoracolumbar/double major/triple major curves. The system also fails to consider a 3-dimensional scope of deformity (4).
Neuromuscular Scoliosis
Some syndromes where scoliosis is likely to happen are connective tissue disorders such as Marfan’s and Ehlers-Danlos syndrome, trisomy 21, Prada-Willi, Retts syndrome and Beale’s syndrome (9).Duchenne muscular dystrophy or spinal muscular atrophy can prevent or severely reduce muscle activation, encourage the development of muscle imbalance, muscle atrophy and progress to spinal scoliotic curvature (9).
Patients with connective tissue related disorders can often develop scoliosis or kyphosis, or both. As they grow and their trunk muscles becomes weaker, the spine gradually begins to collapse, which can create a long, C-shaped collapsing scoliosis (9). Curves are usually progressive which means they continue to grow bigger. For children who use a wheelchair, progressive curves can make it difficult for them to sit comfortably (9). Large curves (measuring 80 degrees or above) in the upper or middle parts of the spine may cause lung problems.
The association of scoliosis with conditions known to be related to collagen abnormalities (e.g. Marfan syndrome) is corroborated by the abnormalities in the amount of collagen associated with low glycosaminoglycan levels in the apical discs
Signs and Symptoms
In the majority of cases, pain is not usually a reason for patients to obtain further medical assistance but patients may present with either back or rib prominence pain (4). Night pain in one constant area is an unusual complaint and should be referred for further imaging to rule out another pathology such as a spinal tumour (4).
Other important features may include balance and gait disturbances, re-duced bowel and bladder control or neurological deficit(s)(4). As Haleem and Nnadi (2018) explain, such revealed symptoms should alert the
examiner to suspect or keep in mind other pathological causes including tumours
(both intra and extradural) and central causes such as syringomyelia (4).
Curve progression needs to be carefully monitored, in
younger children (particularly those less than 10 years of age)
lung volume growth may be impaired and if untreated severe or
progressive scoliosis can lead to or worsen chronic restrictive
respiratory disease .
Treatment
Treatment for scoliosis is based on the type of scoliosis, magnitude of the curve, the number of years of
growth remaining and the patient’s opinion about the shape
of their back (5).The trunk deformity and
balance is also included in the decision-making process(5).
As Janicki and Alman (2017) report, the management and treatment of patients with either congenital,
neuromuscular, syndrome-associated, idiopathic scoliosis or individuals who are younger than 10 years of age presents a number of controversies.
The treatment options for AIS include observation,
bracing and surgery. While many other factors must be considered, the general goal is to keep curves under 50° during maturity (5).
Observation
Typically, observation is recommended for
immature patients with curves less than 25° (5).The most reliable method of monitoring
growth is simple height measurements and primary physicians often possesses this information from their
annual examinations (5).
Braces
Compliance and wearing time of braces seem to have a role in the effectiveness of bracing and although they do not permanently improve or correct spinal curves, they do try to prevent it from worsening (5). Braces include the Milwaukee brace, Boston brace
and the Charleston bending brace (5).
Surgery
Surgery is usually performed during adolescence, but newer techniques have allowed good correction to be
accomplished into early adulthood (5).Surgical correction of idiopathic scoliosis is considered for
curves greater than 45° in immature patients and for curves
greater than 50° in mature patients.
The goals for surgical
treatment include prevention of progression, improve spinal
alignment and balance and help improve alignment between hips and shoulders and the head over the sacrum (5).The spine is corrected with a combination of rods, hooks, screws and wires while being fused by
bone graft either from the patient, a cadaver or artificially. Operative techniques for spinal correction are updated frequently, long-term results have not yet been obtained for the
newest techniques, but good results have been found with older technologies within a 20-year follow-up period (5).
References
- Choudhry, M. N., Ahmad, Z., Verma, R. (2016) Adolescent Idiopathic Scoliosis, The Open Orthopaedics Journal, 10: 143-154.
- Fadzan, M., Bettany-Saltikov, J. (2017) Etiological Theories of Adolescent Idiopathic Scoliosis: Past and Present, The Open Orthopaedics Journal, 11: pp. 1466-1489.
- Francis, M. J. O., Sanderson, M. C., Smith, R. (1976) Skin Collagen in Idiopathic Adolescent Scoliosis and Marfan's Syndrome, Clinical Science and Molecular Medicine; 51: 467-474.
- Haleem, S., Nnadi, C. (2018) Scoliosis: A Review ; 28: 5; 2019 – 217.
- Janicki, J. A., Alman, B. (2017) Scoliosis: Review of diagnosis and Treatment; Orthopaedic Subspeciality Article , 12; 9: 771 – 776.
- Kim, H., Kim, H. S., Moon, E. S., Yoon, C-S., Chung, T-S., Song, H-T., Suh, J-S., Lee, Y, H., Kim, S., (2010) Scoliosis Imaging: What Radiologists Should Know , Radiographics, 1823-1842.
- Koumbourlis, A. C. (2006) Scoliosis and the Respiratory System, Paediatric Respiratory Reviews , Elsevier, 7: 152 - 160.
- Perkins, J., Boyer, A., Mcleish, A., Grossnickle, K. (2013) Idiopathic Scoliosis and Pelvic Floor Dysfunction, IJTR, 19;2:
- Scoliosis Association UK https://www.sauk.org.uk/types-of-scoliosis/syndromic-scoliosis ONLINE
- Scoliosis Research Society, https://www.srs.org/patients-and-families/conditions-and-treatments/parents/scoliosis [Online] Last visited 21/02/2021.
- Stitzel , Clayton. (2017) The Different Scoliosis Locations & Types of Spinal Curvatures [ONLINE], https://www.treatingscoliosis.com/blog/scoliosis-spinal-curvature-types/
- Uden, A., Nilsson, I. M., Willner, S. (1980) Collagen Changes In Congenital And Idiopathic Scoliosis, Acta Orthop. scand; 51: 271-274.


