Tennis Elbow
- by Joanna Blair
- •
- 10 Sept, 2023
- •
Anatomy & Pathology

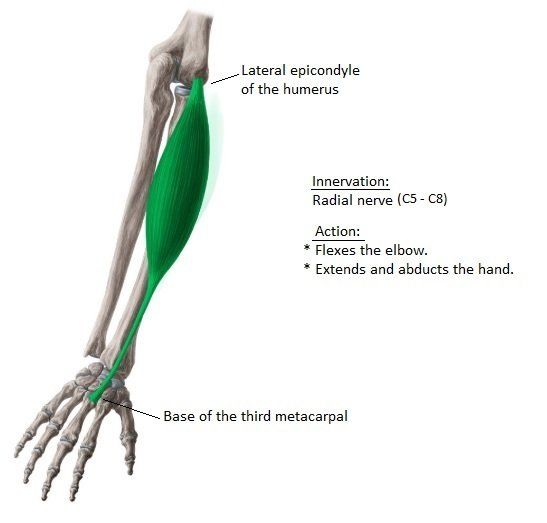
Tennis elbow is also known as lateral epicondylalgia (LE) or lateral epicondylitis, it is a common musculoskeletal condition and mainly affects the extensor carpi radialis brevis (ECRB) muscle (figure 1)(Heales et al., 2016).
Tennis elbow can cause the following symptoms (from NHS guidelines):
- Pain is mainly reported within the outside of the arm.
- Pain that can radiate down into the forearm and wrist.
- Pain when twisting the forearm – for example, when turning a door handle or opening a stubborn lid on a jar.
- Pain and stiffness when fully extending the arm.
- Pain when writing or gripping small objects – for example, when holding a pen.
- Pain when bending of lifting the arm.
Extensor Carpi Radialis Brevis
Prevalence
The condition is equally prevalent in men and women and affects 5-15% of the working population and occurs more commonly in the dominant arm (1).
Symptoms
Pain within the lateral or outer aspect the elbow is the primary symptom of LE and often creates impaired gripping and activities of daily living (ADLs).
Cause
Usually brought about from overuse or a repetitive strain or exertion of the extensor tendons and structures supporting the joint (repetitive strain injury or RSI). It is characterised as microtears, collagen degeneration and angioblastic proliferation for the extensor tendon (1).
Tennis elbow can be caused by physical activity involving gripping or manipulating objects with the hand and can hinder a person's function of their limb during the participation of recreation and occupational activities.
Tennis elbow may also be associated with other related symptoms and complaints such as a painful grip (2).
Magnetic Resonance Imaging (MRI) scan and Imaging
An MRI scan has been previously used to evaluate the degeneration of the common extensor tendon origin in LE patients and has shown that the area corresponds to degeneration and neovascularisation.
The field of view should cover the distal humeral metaphysis to the bicipital tuberosity of the radius. The latter is particularly crucial in known or suspected cases of biceps tendon injury or rupture. Imaging should be performed in all 3 planes, as certain structures are best seen in different planes.
Anatomy
The elbow joint comprises of articulations among 3 bones: the humerus, radius and ulna which allow for flexion (bending of the joint), extension (joint straightening) and supination of the forearm (turning the arm to face the ceiling). The joint capsule is thickened laterally and medially to form the collateral ligament complexes.
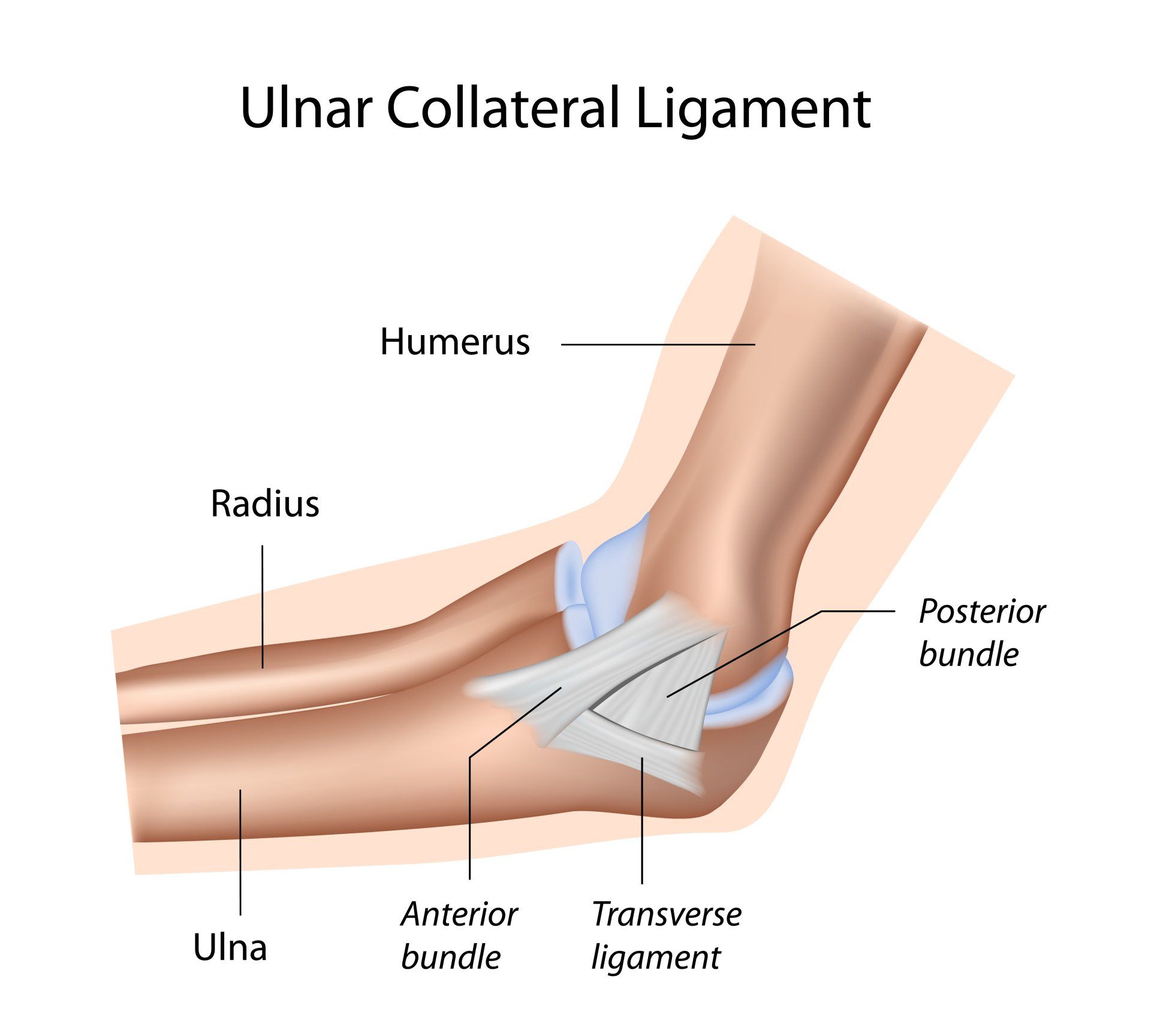
The Ulnar Collateral Ligament (figure 2)
Comprises of 3 bands:
1.) The anterior band is the most important stabiliser and restrains the joint from valgus stress. This aspect of the ulnar collateral ligament extends from the medial epicondyle to the sublime tubercle of the medial base of the coronoid process of the ulna.
2.) The radial collateral ligament which provides varus stability and comprises of 4 parts.
3.) The posterior band which is the least significant transverse band.
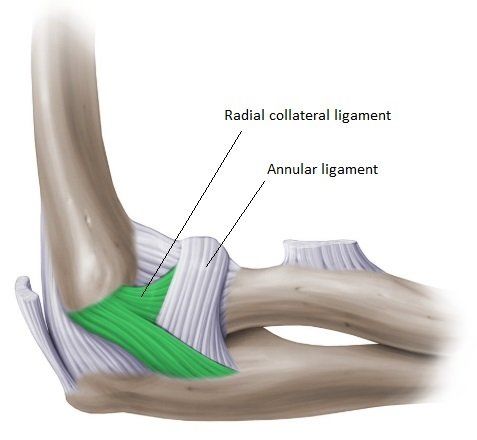
The Radial Collateral Ligament has 4 parts (Sampath et al., 2013:
The radial collateral ligament has a low attachment to the lateral epicondyle of the humerus. The distal fibres blend with the annular ligament that encloses the head of the radius, as well as with the fibres of the supinator and the extensor carpi radialis brevis muscles.
1.) The annular ligament: wraps around the radial head and attaches to the sigmoid notch of the ulna.
2.) The radial collateral ligament: extends from the lateral epicondyle to the annular ligament.
3.) The lateral ulnar collateral ligament (LUCL) runs posteriorly from the lateral epicondyle to the supinator crest of the ulna. Its function is to restrain the elbow joint from varus stress and isolated tearing of the ligament may result to posterolateral rotator instability.
4.) The accessory collateral ligament, which is variably present
The Common Flexor Tendon Groups
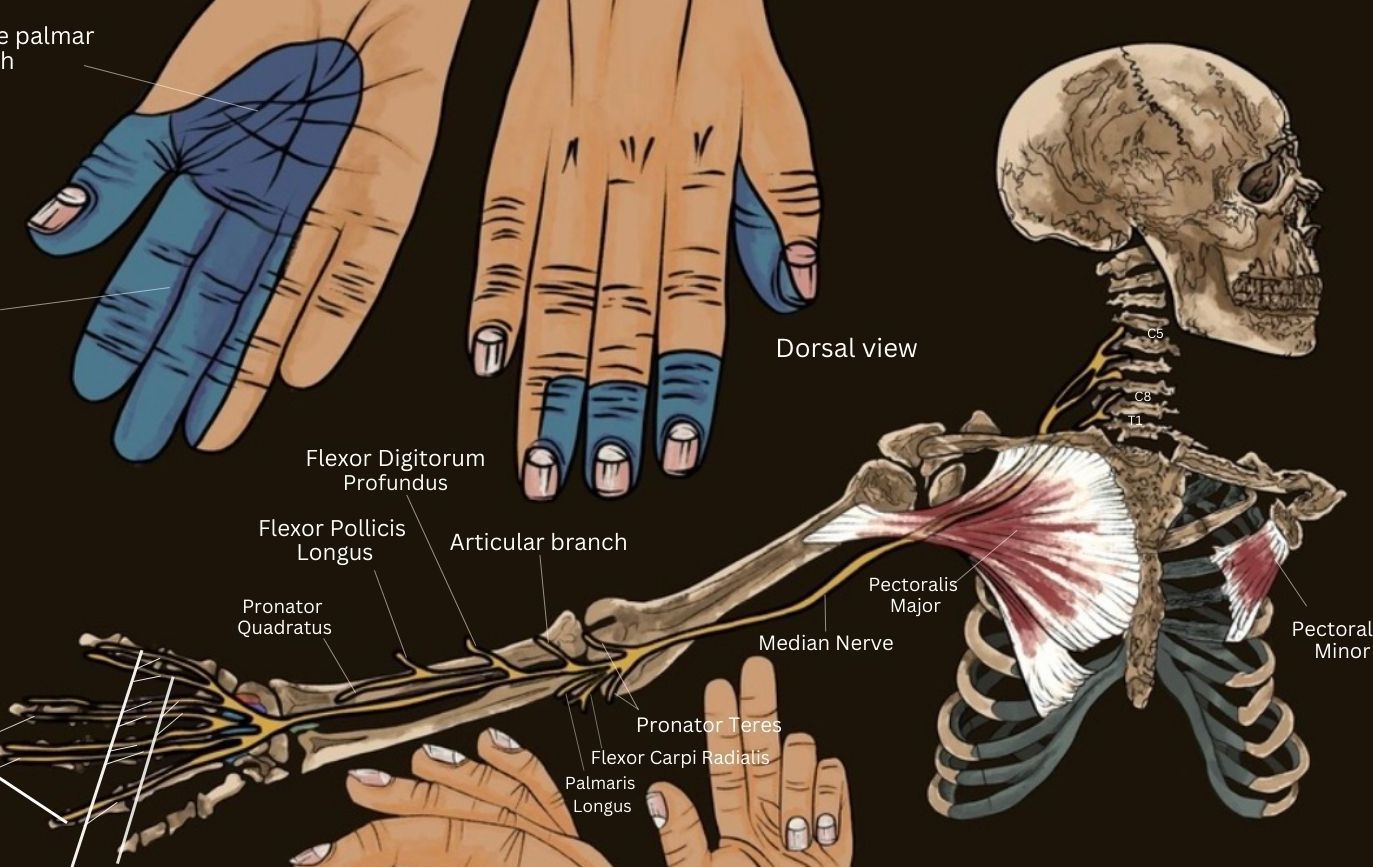
The common flexor tendons comprise of small muscles within the inner, medial muscle group of the arm; the pronator teres, flexor carpi radialis, flexor carpi ulnaris, flexor digitorum superficialis, palmaris longus which insert on the medial epicondyle just proximal to the ulnar collateral ligament.
The common extensor tendon Group:
Comprises tendons of the lateral group muscles; the brachioradialis, extensor carpi radialis longus and brevis, extensor digitorum, extensor carpi ulnaris and the supinator. These insert on the lateral epicondyle.
The anterior muscle compartment includes the biceps brachii and brachialis the posterior group comprises the triceps tendon and anconeus.
The neurovascular structures of the elbow, which are well visualized on MRI, include the ulnar nerve, which takes a superficial course along the posteromedial humerus and lies within the cubital tunnel; the median nerve, which runs in a superficial course posterior to the bicipital aponeurosis (lacertus fibrosus) and anterior to the brachialis muscle; the radial nerve, which is found anterior to the lateral epicondyle, between the brachialis and brachioradialis muscles; and the brachial artery, which runs medial to the biceps tendon in the antecubital fossa.
Pathology & Medical Imaging
Magnetic resonance imaging (MRI) is the modality of choice for the detection of fractures, particularly of the radial head, which are
often suspected on the basis of persistent pain or joint effusion (5).
An magnetic resonance angiogram (MRA) might be useful for partial thickness tears, especially distal deep fibers of the anterior band of the ulnar collateral ligament near its insertion onto the sublime tubercle have been described ashaving a T-shaped appearance (“T sign").
Bone Marrow Edema for Tennis and Golfer’s Elbow
Bone marrow edema can also help to define discrete patterns of injury, which are encountered in both recreational and elite athletes. For instance, both medial epicondylitis (golfer’s. inner elbow pain) and lateral epicondylitis (tennis/ outer elbow pain) can be seen in association with bone marrow edema. In such cases, bone marrow edema can provide a clue for closer scrutiny of tendon or ligamentous injury.
Biceps Tendon
The main distal tendon of the anterior muscle group is the biceps tendon, which inserts onto the radial tuberosity and is involved in both flexion and supination of the forearm. Rupture of the distal biceps tendon is rare, representing less than 5% of all biceps tendon injuries.
Physical Therapy Treatment Options
References
1. Chourasia, A. O., Buhr, K. A., Rabago, D. P., Kijowski, R., Sesto, M. E., (2012) The Effect of Lateral Epicondylosis on Upper Limb Mechanical Parameters, Clinical Biomechanics, Elsevier; 27: 124-130.
2. Heales, L. J., Hug, F., Macdonald, D. A., Vicenzino, B., Hodges, P. W. (2016) Is Syndergistic Organisation of Muscle Coordination Altered in People With Lateral Epicondylalgia? A Case-Control Study, Clinical Biomechanics, Elsevier; 35: 124-131.
3. Kijowski, R., Tuite, M., Sanford, M., 2005. Magnetic resonance imaging of the elbow. Part II: Abnormalities of the ligaments, tendons, and nerves. Skeletal Radiol. 34, 1–18.
4. NHS, https://www.nhs.uk/conditions/tennis-elbow/symptoms/
5. Sampath S. C., Sampath, S. C., Bredella, M. A. (2013) Magnetic Resonance Imaging of the Elbow: A Structured Approach, 5: 1; 34-49.